To request a copy of your child's records to be sent to another office, please fill out the form below and fax or email it to the appropriate location.
Harrisburg location - Fax - 717-558-9844 Email - [email protected]
Mechanicsburg location - Fax - 717-737-2158 Email - wes[email protected]
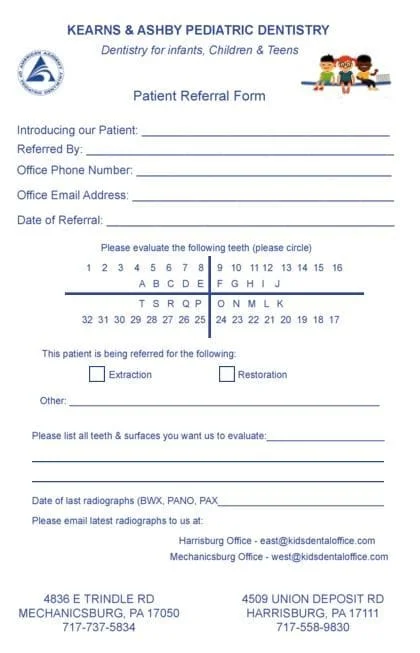
If you would like to refer a patient to our office please click to print the form below and email it along with any current radiographs.
REFERRAL FORM